
Proper gingival retraction is the silent precondition of an accurate impression. The cord by itself mechanically widens the sulcus, but without an astringent agent the sulcular fluid and blood remain a problem that will ruin even the most carefully taken impression. And the choice of impregnating solution is not merely a question of hemostasis – it influences the biological response of the tissue, the quality of the preparation surface, and what is left behind on the tooth after the cord is removed.
01OverviewHow Astringent Agents Work
Astringent substances act by local vasoconstriction or precipitation of proteins in the sulcular fluid, thereby stopping bleeding and reducing secretion. The result is a dry, open sulcus into which the impression material can reliably flow all the way down to the margin of the preparation.
Four main groups are used clinically:
- Aluminum chloride (AlCl₃) – the most widely used choice, at concentrations of 10–25%. It acts quickly, is gentle to the tissue, and after rinsing leaves no visible residue on the tooth surface. Studies comparing different retraction methods have confirmed that a cord impregnated with aluminum chloride achieves impression quality comparable to modern cordless systems.
- Aluminum sulfate (Al₂(SO₄)₃) – a mechanism similar to AlCl₃, with a slightly higher astringent effect. Available in both gel and paste form for the cordless technique.
- Ferric sulfate (Fe₂(SO₄)₃) – a strong hemostatic effect, but it leaves a characteristic brownish-black discoloration on the hard dental tissues as well as on the gingiva. Its oxidative reaction with blood produces precipitates that must be thoroughly removed before taking the impression, otherwise they interfere with the polymerization of addition silicones.
- Epinephrine (adrenaline) – historically used for its pronounced vasoconstriction. It is now being abandoned because of systemic cardiovascular risks, especially in patients with hypertension or ischemic heart disease.
02Tissue ResponseWhat Happens Beneath the Surface
The biological compatibility of astringent agents has been tested on primary human gingival fibroblasts. The results show that preparations based on aluminum chloride, aluminum sulfate, and ferric sulfate do not reduce the viability or proliferation of fibroblasts at clinically relevant concentrations. Only one of the tested preparations (Expasyl, based on AlCl₃ in paste form) induced measurable oxidative stress – an increase in nitrite levels – without any impact on cell survival.
Older studies on fibroblasts confirmed that ferric sulfate exhibits higher cytotoxicity than aluminum chloride on direct contact with tissue – especially with a longer application time or when the sulcular epithelium is injured by the cord.
03Traces on the ToothWhich Agent Leaves the Fewest
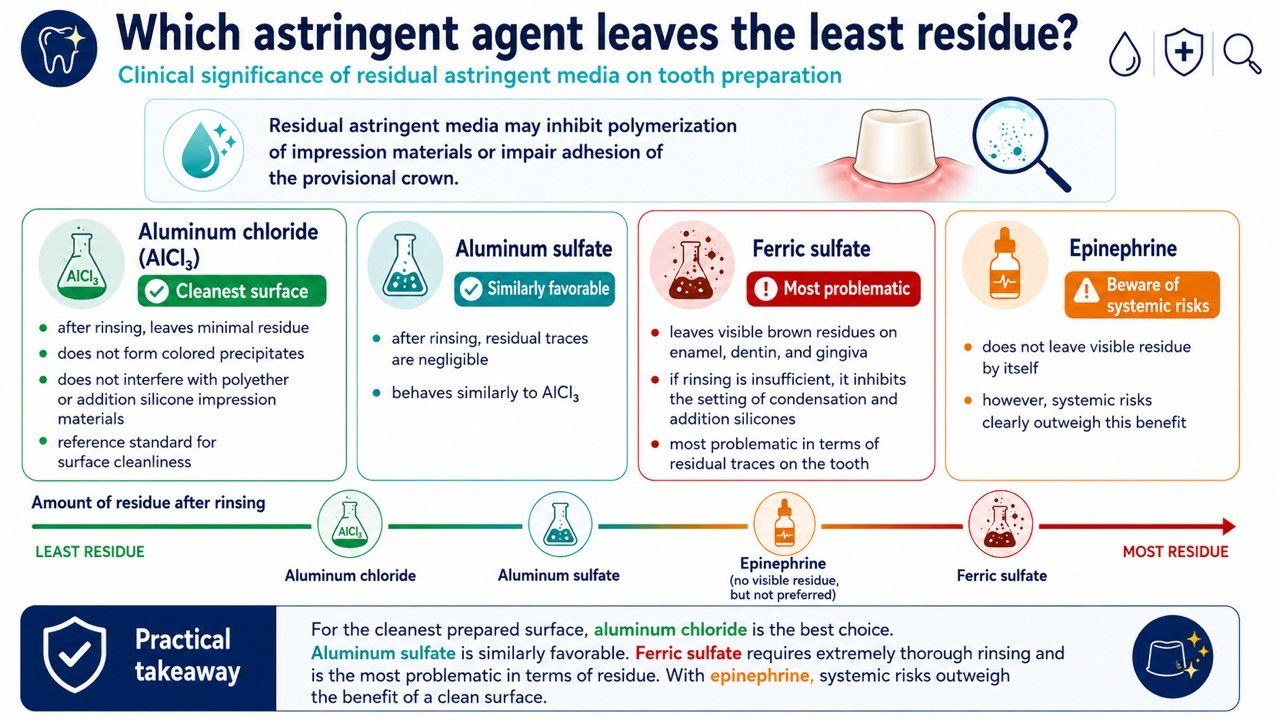
This question has a direct clinical impact: residues of the astringent agent on the preparation can inhibit the polymerization of impression materials or compromise the adhesion of a temporary crown.
- Aluminum chloride leaves minimal residue after rinsing. It does not form colored precipitates and does not interfere with polyether or addition silicone materials. It is considered the reference standard for surface cleanliness.
- Aluminum sulfate behaves similarly to AlCl₃ – residues are negligible after rinsing.
- Ferric sulfate leaves visible brown residues on enamel, dentin, and gingiva. With inadequate rinsing it inhibits the setting of both condensation and addition silicones. In terms of traces on the tooth, it is the most problematic.
- Epinephrine does not by itself leave visible residue, but the systemic risks of its use considerably outweigh this benefit.
04Practical RecommendationWhat to Choose and When
The choice of astringent agent depends on the clinical situation, but the general hierarchy is clear:
- Standard choice: aluminum chloride 15–25% – the optimal balance of hemostasis, tissue gentleness, and surface cleanliness. Suitable for most clinical situations.
- Heavy bleeding: ferric sulfate is effective, but it requires careful rinsing and mechanical cleaning of the preparation before taking the impression. Consider whether it is not better to postpone the impression and treat the cause of the bleeding.
- Cordless systems: gels and pastes based on AlCl₃ or Al₂(SO₄)₃ (e.g., Expasyl, Traxodent) offer impression quality comparable to the cord technique and are faster to apply.
- Epinephrine: unsuitable for cardiovascular-risk patients; in modern practice replaced by safer alternatives.
Gingival displacement is a critical step in fixed prosthodontics — the choice of chemical agent directly affects both tissue health and impression accuracy.
Baba N.Z. · Dental Clinics of North America, 2014
Regardless of the agent chosen, one rule holds: before taking the impression, always rinse thoroughly, suction, and visually inspect the surface of the preparation. No astringent agent can replace careful technique.

🌍 Cicero System🎓 Dental Education | 🛒 Procurement | 🏥 Clinic Management