
In law firms it is taken for granted: a senior partner brings in a talented junior, offers them a stake after a few years, and the firm keeps growing — without anyone having to leave and start their own practice from scratch. In the dental world this model barely exists. And yet the logic is exactly the same.
01Why It Works for LawyersAnd Why Not for Dentists
Law firms are built on a simple truth: the best people leave if you don't offer them the prospect of ownership. The partnership model is therefore primarily a tool of retention and motivation — not just a way to divide profit.
In dental practices this approach has not yet spread very far, for several reasons. Practice owners fear a loss of control. Associates don't know how to value a stake. And no one has a ready set of rules under which the agreement could be concluded. The result? Good doctors leave after five years and open their own office — and you start over.
02The Basic ArchitectureWhat a Partnership Looks Like in Practice
The partnership model in a dental practice can take several forms. The three most common are:
- Equity partnership — the associate gradually buys a stake in the limited company (s.r.o.) or other legal form of the practice. They become a co-owner of the real estate, the equipment, and the goodwill.
- Operating partnership — the associate does not acquire an ownership stake but receives a share of the profit and decision-making authority in defined areas (recruitment, purchasing, development).
- Hybrid model — a combination of both. The associate starts with a share of the profit and, after meeting the conditions (length of cooperation, turnover, patient base), transitions to an equity stake.
Each of these models works — provided the rules are clear. If they are not, each of them leads to conflict.
03What the Agreement Must AddressSeven Points You Can't Do Without
Lawyers treat the partnership agreement as standard. Dentists mostly don't have one at all. And yet it is enough to cover seven basic areas:
- Entry conditions — what the associate must fulfill in order to obtain the partnership (years of practice, turnover, performance reviews).
- Valuation of the stake — how the value of the practice is calculated at the moment of entry (EBITDA multiple, goodwill, equipment).
- Financing method — does the associate buy the stake out of future profits, or take out a loan? Who guarantees it?
- Profit distribution — how the operating profit is divided among the partners (equally, by turnover, by stake)?
- Decision-making authority — what each partner can decide alone and what requires the consent of both?
- Exit clause — what happens when one partner wants to leave, dies, or becomes incapacitated?
- Non-compete — for how long and within what radius the departing partner may not run a competing practice?
Most disputes between partners do not arise from ill will. They arise because each one remembers the verbal agreement differently.
Zkušenost z praxe — právní poradenství pro zdravotnická zařízení
04How to Set It Up Step by StepFrom Associate to Partner
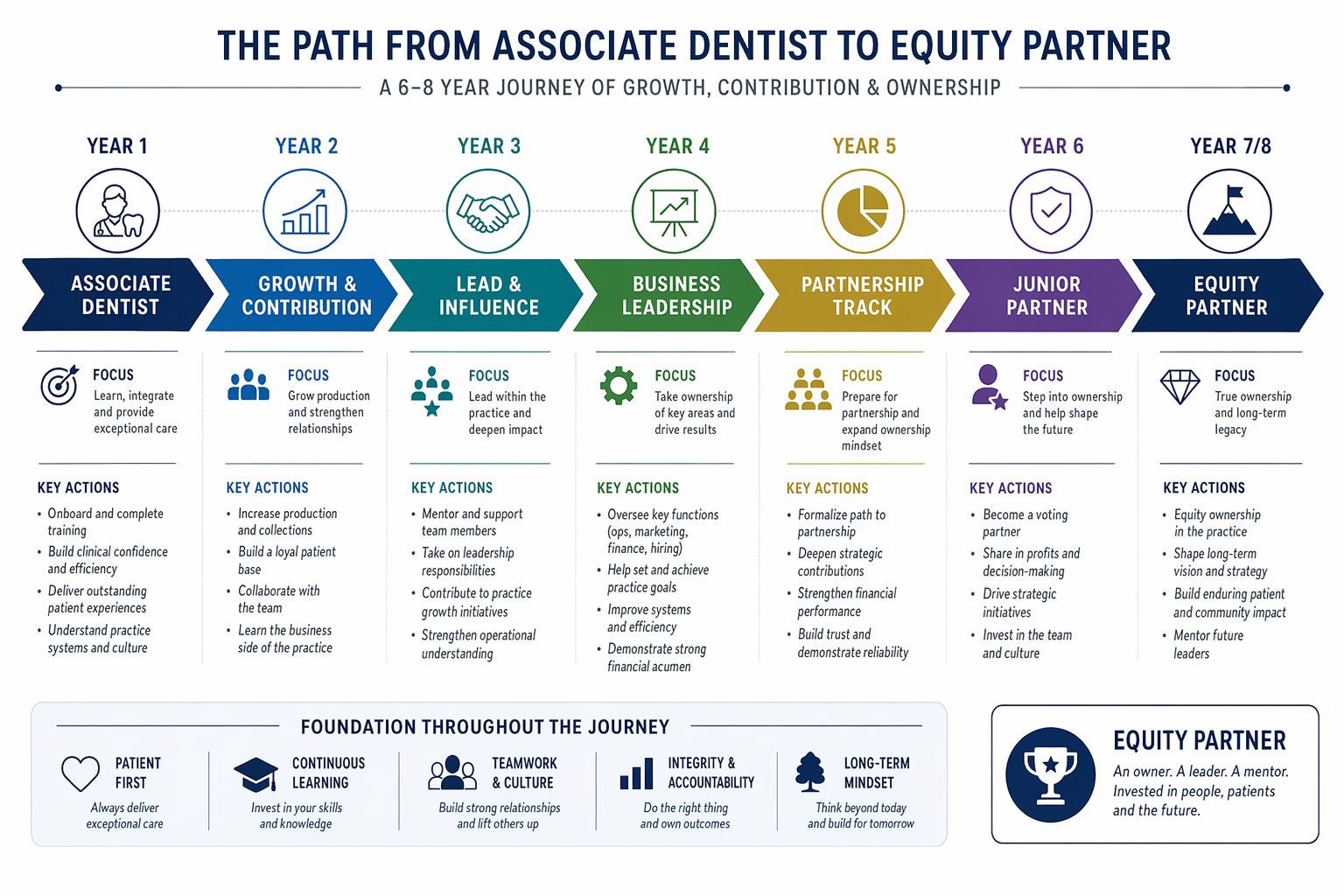
The best-functioning models have a clear timeline. An example that can be adapted:
- Years 1–2: The associate works under a standard contract, builds a patient base, and learns the culture of the practice.
- Year 3: A formal review — turnover, patient satisfaction, teamwork. If the criteria are met, negotiations on the partnership begin.
- Year 4: Signing of the partnership agreement, the first equity entry (typically a 10–25% stake).
- Years 6–8: The option to increase the stake based on conditions agreed in advance.
The key point is that the whole path is defined in advance — the associate knows from day one what lies ahead and what is expected of them. That in itself changes the dynamic of the relationship.
05When It Doesn't Make SensePartnership Isn't for Everyone
The partnership model is not a universal solution. It does not make sense if:
- The practice is too small (one dentist, one surgery) — the added value of partnership won't cover the administrative costs.
- The owner plans to sell the practice within 3–5 years — bringing in a partner complicates the exit.
- The associate has no interest in ownership — some doctors simply want to do good work and earn well, without entrepreneurial risk. That is a legitimate choice.
Partnership works where both sides want to build something together over a longer horizon — and where both are willing to invest the time in setting up the rules.
Dental practices that introduce the partnership model have lower doctor turnover, higher team engagement, and a stronger position in the event of a sale or expansion. It is not complicated — but it does take the courage to sit down at the table and agree on the numbers before the first conflict arrives.

🌍 Cicero System🎓 Dental Education | 🛒 Procurement | 🏥 Clinic Management