
The extraction of a mandibular third molar is one of the most common procedures in dental surgery. At the same time, it is a procedure after which the patient comes back with a question that has no easy answer: "Why did my tongue go numb?" or "When will my lip stop tingling?" Injury to the n. lingualis and the n. alveolaris inferior is not a rarity — it is a predictable complication that can be managed, if we know what to look for.
01AnatomyWhy Both Nerves Are So Vulnerable
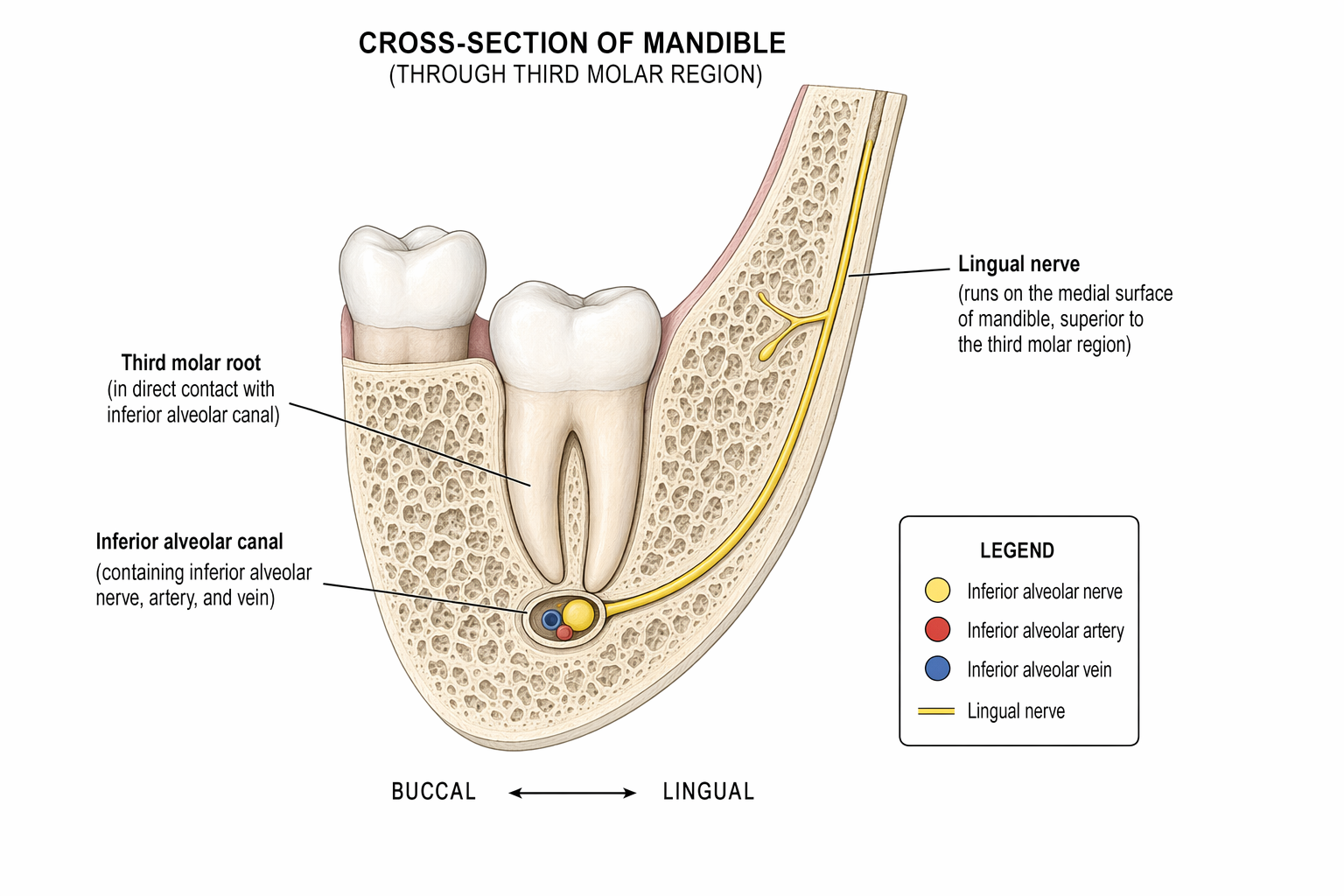
The n. alveolaris inferior (IAN) enters the foramen mandibulae and runs through the canalis mandibulae just below the roots of the mandibular molars. In deeply impacted third molars, the distance between the root apex and the wall of the canal may be zero — the nerve lies literally in contact with the root. A panoramic radiograph reveals warning signs: loss of the cortical line of the canal, darkening of the root at the point of overlap, or narrowing of the canal. These signs have high sensitivity for predicting contact, but low specificity for predicting an actual injury.
The n. lingualis descends medially from the m. pterygoideus medialis and, in the region of the third molar, lies subperiosteally on the lingual side of the mandible — in some anatomical variations even above the alveolar crest, without any bony protection. This is precisely why it is vulnerable during elevation of the lingual flap, when a lingual retractor is used, or during aggressive dissection in this space.
02ClassificationNeurapraxia, Axonotmesis, Neurotmesis — Why It Matters
Seddon's classification (1943) divides peripheral nerve injuries into three grades and directly determines both prognosis and management:
Neurapraxia is the mildest form. The axon is intact; only conduction is interrupted — most often by pressure, traction, or transient ischemia. The patient describes hypoesthesia or paresthesia, but function recovers spontaneously, typically within 8–12 weeks, exceptionally within 6 months. This is the most common type of injury after a third-molar extraction.
Axonotmesis means interruption of the axon with the endoneural tube preserved. Regeneration proceeds at a rate of approximately 1 mm/day, but the outcome depends on the length of the damaged pathway. Recovery takes months and may be incomplete.
Neurotmesis is complete transection of the nerve, including the connective tissue. Spontaneous regeneration is minimal or absent. Without microsurgical intervention, a permanent deficit is likely.
Neurapraxia is a functional block without structural damage to the axon — conduction is restored spontaneously once the cause subsides.
Seddon HJ · Brain, 1943
In practice, the type of injury cannot be reliably distinguished clinically immediately after the procedure. The key is monitoring the dynamics of the symptoms over time.
03SymptomsHow the Injury Presents and How to Distinguish It
IAN injury manifests on the lip, chin, and mucosa of the mandibular vestibule on the ipsilateral side. Injury to the n. lingualis affects the anterior two-thirds of the tongue (touch, heat, cold) and — which patients perceive as particularly disturbing — taste on the ipsilateral side, because the chorda tympani runs within the sheath of the n. lingualis.
Typical symptoms:
- Hypoesthesia — reduced perception of touch, temperature
- Paresthesia — tingling, pins and needles without an apparent stimulus
- Dysesthesia — unpleasant or painful perception of a normally non-painful stimulus (allodynia)
- Taste disturbance (ageusia, dysgeusia) — specific to the n. lingualis
- Neuropathic pain — burning, shooting, spontaneous; a more serious form that requires specialized care
The differentiation is straightforward: lip and chin = IAN, tongue and taste = n. lingualis. Combined symptoms are rare but possible with more extensive traumatization.
04Risk Factors and PreventionWhat We Know from the Literature
Systematic reviews consistently identify the following risk factors for IAN injury: older patient age, fully developed roots, deep impaction (Pell-Gregory III), radiographic contact of the root with the canal, a difficult operation, and intraoperative exposure of the nerve. The incidence of transient IAN dysesthesia in the literature ranges around 3–4 %, while permanent dysesthesia persists in fewer than 1 % of patients. Injury to the n. lingualis is less common (around 2 %), but permanent damage is rare (below 0.5 %).
Preoperative imaging: The panoramic radiograph (OPG) is the standard. Warning signs on OPG (loss of the cortical line of the canal, darkening of the root, deviation of the canal) indicate CBCT. CBCT depicts the bucco-lingual relationship of the root and canal more accurately and makes it possible to identify a lingual course of the canal — which is associated with a higher risk of injury. However, studies show that CBCT, compared with OPG, does not statistically significantly reduce the incidence of postoperative neurological complications in moderate-risk cases — its benefit lies in more accurate planning of the surgical approach, not in elimination of the risk as such.
Surgical technique: The lingual flap should not be elevated without indication. If it is necessary, the lingual retractor must be placed gently and without excessive pressure. Osteotomy should be carried out so as to minimize the transmission of vibration and heat to the canal region. Coronectomy (intentional retention of the roots) is a valid alternative in high-risk cases with direct contact between the root and the IAN.
05CorticosteroidsPreventive Administration in a Demanding Operation
Corticosteroids are an established method in oral surgery for reducing postoperative swelling, trismus, and pain. Their role in protecting the nerve is indirect: they reduce perineural edema, which can prolong or deepen neurapraxia.
When to indicate them: In extractions expected to be demanding (deep impaction, an anticipated long operating time, radiographic contact with the IAN), the preventive administration of a corticosteroid is justified.
Therapeutic window: The corticosteroid must be administered before or immediately after the procedure — ideally within 24 hours of the operation, no later than 72 hours. After 72 hours, the anti-inflammatory effect on acute perineural edema is minimal.
Dexamethasone is the preparation of choice for single or short-term administration:
- Standard dose: 8 mg dexamethasone i.m. or i.v. immediately before the procedure or immediately after it
- Alternatively oral: 8 mg on day 0 (the day of surgery), 4 mg on the morning of day 1, 4 mg on the morning of day 2 — 3 days in total
- For very demanding procedures, a 3-day tapering schedule can be considered: 8–4–4 mg p.o.
Methylprednisolone is an alternative, especially when the goal is the reduction of trismus:
- 40 mg i.m. or 32 mg p.o. on the day of surgery, optionally a 2–3-day tapering schedule
- A 2025 meta-analysis (Libório et al.) showed that methylprednisolone is more effective than dexamethasone in reducing trismus (inter-incisal distance), while dexamethasone has a slight advantage in reducing swelling.
What to watch out for:
- Corticosteroids are contraindicated in uncontrolled diabetes, active infection (pericoronitis with systemic symptoms), immunosuppression, an active peptic ulcer, and in patients on anticoagulant therapy (relative contraindication — increased risk of bleeding)
- Single or 2–3-day administration is safe in healthy patients; systemic adverse effects are minimal with such short administration
- Corticosteroids do not treat nerve injury — they reduce the inflammatory component that can complicate the course of neurapraxia
06Communicating with the Patient"The Nerve Isn't Dead, Just Annoyed"
A patient who wakes up with a tingling lip or a numb tongue is frightened. The way you explain the situation to them in the first few minutes determines whether they will cooperate — or whether they will come back a year later with a lawyer.
If the clinical picture corresponds to neurapraxia (hypoesthesia without pain, without progression, in a distribution corresponding to a single nerve, immediately after the procedure), it is appropriate to tell the patient something like this:
"The nerve was not severed. It is irritated — like when you sit on your leg and can't feel it for a while. Signal conduction is temporarily blocked, but the structure of the nerve is preserved. In most patients, sensation returns within 8–12 weeks; in some, recovery takes up to 6 months. We will monitor it."
This formulation is clinically accurate for neurapraxia and at the same time understandable. Do not use it if you suspect a more serious injury (severe dysesthesia, neuropathic pain, no tendency toward recovery after 3 months).
Documentation and informed consent: The risk of nerve injury must be part of the informed consent before every extraction of a mandibular third molar. The consent must be written, dated, and signed. Document the preoperative neurological status (normal sensation of the lip and tongue), the imaging methods used, the operative findings, and the postoperative neurological assessment at each follow-up.
07Follow-Up and ReferralWhen to Say "I Can't Handle This Alone"
The postoperative check-up should include a simple neurological examination: touch with a cotton swab on the lip, chin, and tongue, compared with the healthy side. Record the result in the documentation.
When to refer to a specialized center (oral and maxillofacial surgery, neurology):
- No tendency toward recovery after 3 months from the procedure
- Progressive or newly arising neuropathic pain (dysesthesia, allodynia)
- Suspicion of neurotmesis (complete anesthesia without any sign of recovery)
- N. lingualis injury with a taste disturbance persisting longer than 6–8 weeks
- A patient who does not agree to conservative monitoring and requests active intervention
Microsurgical nerve reconstruction (neurorrhaphy, interpositional graft) has the best outcomes if it is performed within 3–6 months of the injury — which is why early referral is crucial. After 9–12 months, the success rate of reconstruction declines markedly.

🌍 Cicero System🎓 Dental Education | 🛒 Procurement | 🏥 Clinic Management