
The preventive check-up is the most frequent procedure in dental practice – and the one most often documented inadequately. Yet prevention is exactly where you catch things the patient would never spot on their own: early periodontitis, mucosal lesions, the first signs of an oncological disease. For the check-up to actually do its job, it needs structure.
01The basicsWhy you need a firm prevention protocol
An improvised "eyeball" check isn't prevention – it's just a look at what is visible at first glance. A firm protocol ensures every patient receives the same level of care regardless of how busy the practice is or who performs the examination.
The protocol has another dimension: legal. The medical record must demonstrate that care was provided lege artis. If the record is missing, say, the mucosal examination or the periodontal screening, you cannot show they were performed – and in a dispute, what is not recorded counts as not done.
02What to recordThe required content of the medical record at a check-up
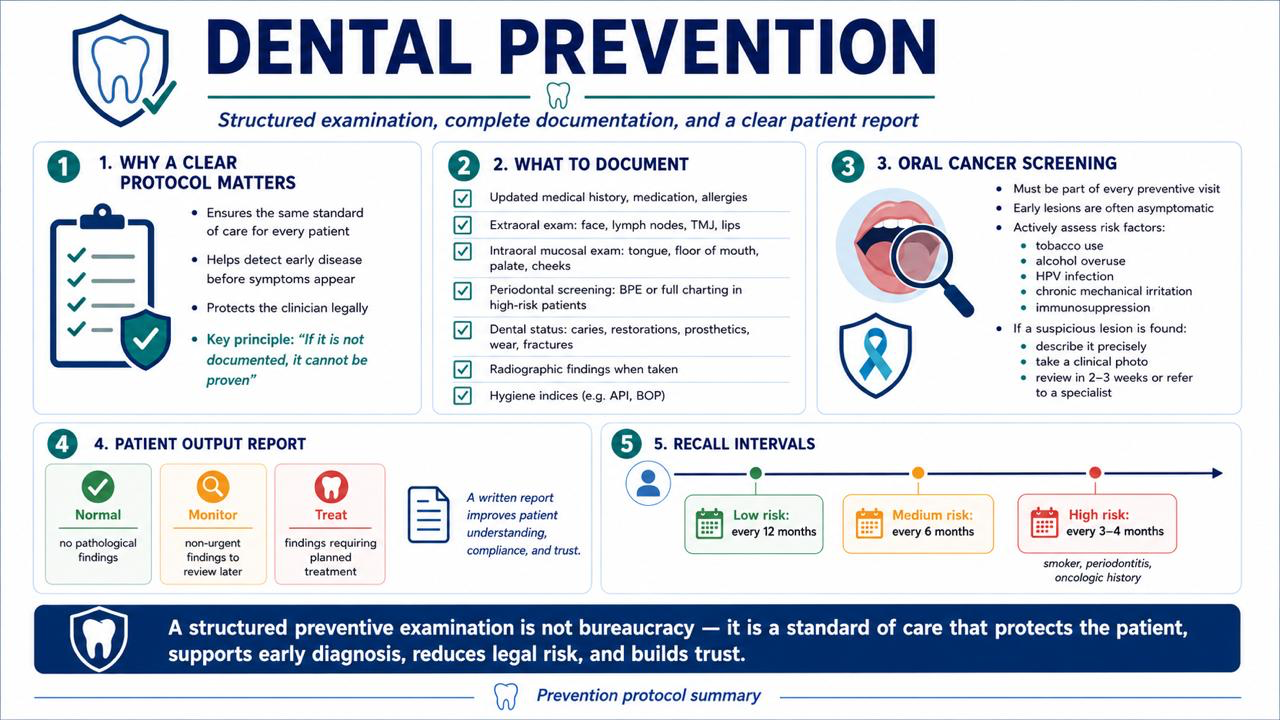
Documenting a preventive check-up has to contain more than "no complaints, follow-up in 6 months". Below are the areas that must be present:
History and health-status update – at every check-up confirm whether the general health status, medication or allergies have changed. Record the date of the update and the patient's signature.
Extraoral examination – facial symmetry, lymph nodes of the neck and submandibular region, temporomandibular joints (crepitation, limited opening), lips.
Intraoral mucosal examination – systematically: vestibule, buccal mucosa, tongue (dorsum, lateral borders, ventral surface), floor of the mouth, palate, tonsillar region. Every deviation must be described by location, size, colour and surface character.
Periodontal screening – at minimum BPE (Basic Periodontal Examination) or a full periodontal chart for risk patients. Record bleeding on probing, pocket depths, furcation involvement.
Dental status – current state of the dentition, presence of carious lesions, the state of existing fillings and prosthetic work, abrasion, erosion, fractures.
Radiographic finding – if an image was taken, record the type, date and conclusion.
Hygiene index – an objective record (e.g. API, BOP), not just a subjective rating.
Oncological screening – see the dedicated section below.
03Oncological preventionPart of every check-up, not the exception
Oral carcinoma is diagnosed late in more than 60% of cases – precisely because early lesions are asymptomatic and the patient doesn't notice them. The dentist is in a unique position: they see the mucosa regularly and systematically, which no other specialist does.
Oncological screening must be part of every preventive check-up, not only "when something looks suspicious". A systematic examination of the mucosa during prevention catches potentially malignant lesions (leukoplakia, erythroplakia, submucosal fibrosis) at a time when treatment is still curative.
Risk factors that must be actively elicited and documented:
- Smoking and tobacco chewing
- Excessive alcohol consumption
- HPV infection (especially in younger patients with oropharyngeal lesions)
- Chronic mechanical irritation (an ill-fitting prosthesis, a sharp tooth)
- Immunosuppression
Examination of the oral cavity and neck must be part of every dental check-up. Dentists and dental hygienists are effective clinicians for detecting oral cancer.
MacCarthy et al. · Journal of the Irish Dental Association, 2011
If you find a suspect lesion, document it precisely, take photographic documentation and set a clear plan: monitoring with a recall in 2–3 weeks, or direct referral to a specialist.
04The patient hand-outWhy give it and what it must contain
A hand-out for the patient isn't just a polite gesture – it is a tool that boosts compliance and strengthens trust in the practice. A patient who leaves with a written summary of their status better understands why they should return for a check-up or treatment.
The hand-out should be brief, comprehensible and structured into three clear categories:
1. All clear – areas where no problem was found (e.g. "mucosa without pathological findings, periodontium stable").
2. Monitor – findings that are not acute but require attention at the next check-up (e.g. "early abrasion of anterior teeth, change in brushing technique recommended; monitor lesion on the left lateral border of the tongue – recall in 3 weeks").
3. Treat – specific procedures to be scheduled, with an indicative order of urgency (e.g. "caries tooth 36 – treatment recommended within 4 weeks; replace old amalgam filling tooth 14 – plan at the next visit").
Handing over the hand-out also protects the clinician: the patient cannot claim they weren't informed of a finding if they have a written record with date and signature.
05How to introduce this in practiceConcrete steps for your team
Introducing a structured prevention protocol does not require a large investment – it requires a decision and discipline.
- Create a template for documenting the preventive check-up that covers all the areas listed above. The template can be paper or electronic – what matters is that it is always at hand and that nobody deviates from it.
- Standardise the hand-out for the patient. A one-page form with the practice logo, date, patient name and three columns (all clear / monitor / treat) is enough. The clinician fills it in during the check-up or immediately after.
- Train the whole team – the assistant must know what to prepare so the check-up can run systematically (probe, mirror, periodontal probe, sufficient lighting).
- Photographic documentation of suspect lesions should be the standard, not the exception. A photo taken at the first visit allows objective comparison at follow-up.
- Adjust the check-up interval to the patient's risk profile: low-risk patient – 12 months, moderate-risk – 6 months, high-risk (smoker, periodontitis, oncological history) – 3–4 months.
A preventive check-up done according to a clear protocol, properly documented and finished with a hand-out for the patient – that isn't bureaucracy. That is the standard of care that protects the patient, protects the clinician and builds a practice patients trust.

🌍 Cicero System🎓 Dental Education | 🛒 Procurement | 🏥 Clinic Management