
Every clinician knows the moment: a patient refuses recommended care, or alternatively agrees to a procedure that carries risks. In both cases you reach for a piece of paper. But which one? Confusing an informed refusal with an informed consent isn't just an administrative slip — in a dispute, it can decide whether the court stands with you or not.
01Informed consentWhen and why a patient signs it
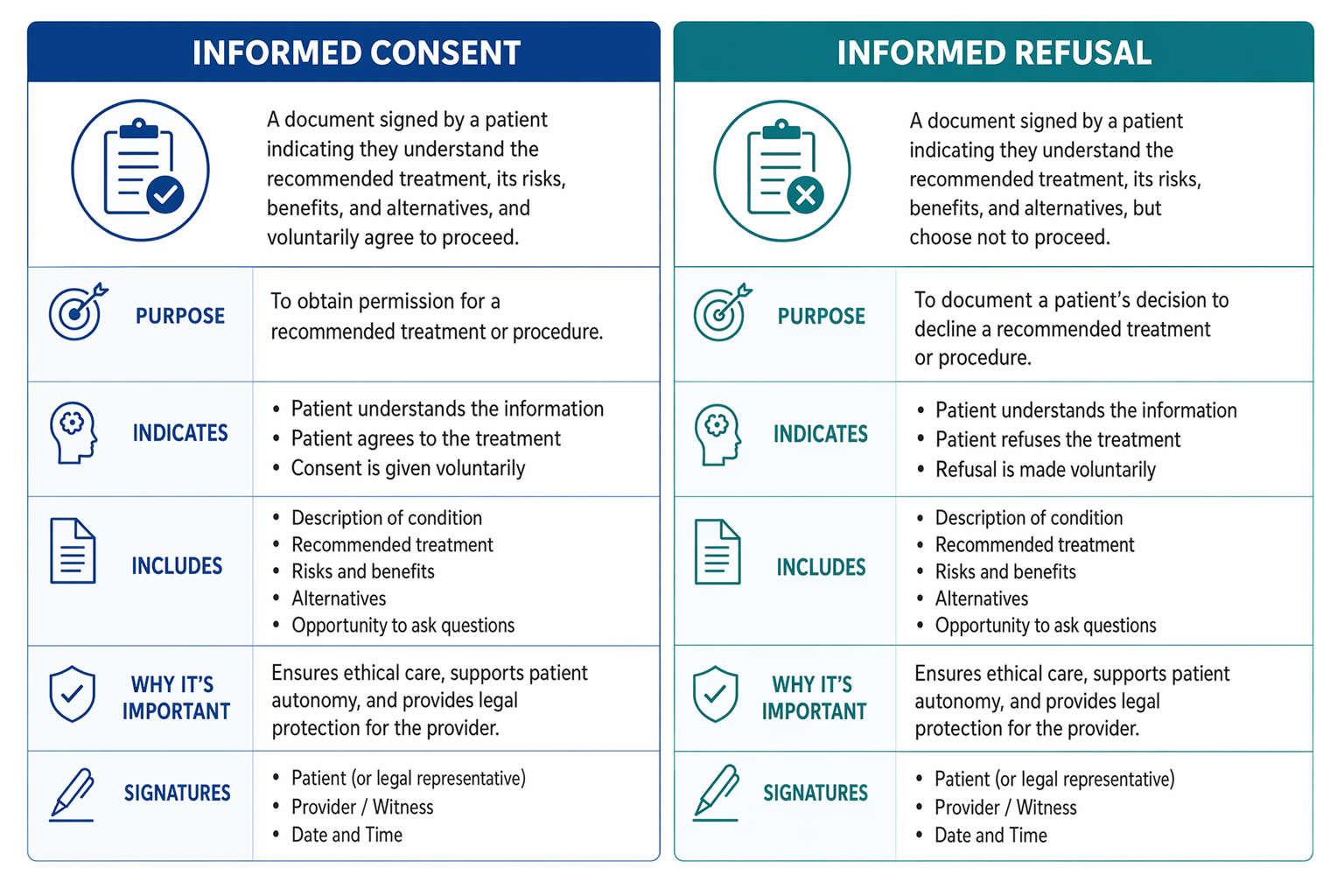
Informed consent is both the legal and the ethical foundation of every medical procedure. Through it, the patient confirms that they were given a clear explanation of the nature of the procedure, its benefits, risks, alternatives and the consequences of not treating — and that they freely agree to the procedure.
It is signed before every invasive or risk-relevant procedure: before an extraction, implant, surgical intervention, anaesthesia, but also before placing fixed orthodontic appliances or larger prosthetic rehabilitation. The consent must be informed, voluntary and given before the procedure starts — a signature "on the way in" or retroactively is not enough.
The key word is informed: it isn't enough that the patient signed a form. You must be able to show that the briefing actually happened — ideally a note in the record, with date, signature and a brief description of what was explained.
02Informed refusalWhen the patient declines what you recommend
An informed refusal is the exact opposite. Through it, the patient declines the proposed procedure or treatment, although they were properly informed of the consequences. In practice, it is the documentary proof that you, as the clinician, fulfilled your duty to inform, the patient acknowledged it, and refuses treatment anyway.
Typical situations where an informed refusal applies:
- The patient refuses extraction of a tooth with infaust prognosis and insists on keeping it.
- They refuse an antibiotic course after a surgical procedure.
- They decline a recommended X-ray or CBCT scan.
- They don't show up for follow-up and decline monitoring.
- They refuse general anaesthesia and insist on local, even though the procedure can't be performed safely under local.
An informed refusal does not automatically release the clinician from responsibility — like a consent, it must be backed by a demonstrable briefing. If a patient signs a refusal without understanding what they are declining, its legal weight is questionable.
The patient has the right to refuse care. The clinician has the duty to clearly explain the consequences of that refusal and to document the refusal.
The principle of patient autonomy.
03The legal weight of both documentsWhat stands up in court
Both documents have legal weight — but different and conditional. A signed sheet of paper isn't enough. A court will examine:
For informed consent:
- Was the patient briefed clearly and with sufficient lead time (not pushed under pressure just before the procedure)?
- Was the consent voluntary — without coercion?
- Does the content of the form actually correspond to the procedure that was performed?
- Is there a record of the briefing, not just a signature?
For informed refusal:
- Was the patient briefed about the specific risks of refusal (not just generic ones)?
- Does the record state what was refused and why?
- Was the patient legally capable of decision-making at the time of signing?
Practice shows that generic forms with pre-printed text the patient signs without a conversation have low evidentiary value in court. By contrast, a brief handwritten note by the clinician in the chart — "patient briefed on the risk of infection spread from refusing extraction, refusal signed on…" — is strong evidence.
04The most common mistakes in practiceWhat gets clinicians into trouble
Mixing up or misusing these documents is among the most frequent administrative failures in dental practice. Specifically:
- Using consent in place of refusal — the patient declines a procedure but signs a "consent to treatment" that doesn't actually decline anything. In a dispute, you have no proof of the refusal.
- A signature without a briefing — the form is signed in the waiting room without a conversation with the clinician. A court will call this a formality without legal relevance.
- Text that is too generic — "I consent to treatment at the XY practice" does not substitute for consent to a specific procedure.
- Missing date or clinician signature — a document without a date is hard to prove.
- A refusal without a chart entry — a signature on a loose sheet without a corresponding record in the documentation is easily contested.
A properly maintained medical record — including both types of document — is your strongest defence in a court dispute. Dental malpractice research repeatedly confirms that the absence or poor quality of documentation is one of the main factors deciding the outcome against the clinician.

Tým za platformou Cicero. Píšeme o digitalizaci ordinací, klinickém workflow a o tom, jak technologie mění každodenní praxi.