
Walk into a dental practice in 1990 and you would find a dental chair, a handpiece, an X-ray unit, and a set of hand instruments. The overhead was real, but it was bounded. Walk into a well-equipped practice today and you are looking at a CBCT scanner, an intraoral scanner, a CAD/CAM milling unit, a digital radiography system, an intraoral camera, a laser, an apex locator, an electric handpiece system, and a practice management platform. Every single one of those devices carries a purchase price, a maintenance contract, a depreciation curve, and a training cost. The question is no longer whether technology raises the cost per minute — it clearly does. The question is by how much, and whether the math still works in the practice's favour.
01The 1990 BaselineWhat a Practice Actually Cost to Run
A general dental practice in 1990 operated with a capital equipment footprint that was modest by today's standards. Conventional film radiography required a processor and film stock. Impressions were taken in alginate or polyvinylsiloxane and sent to an external lab. Sterilisation meant an autoclave. The dominant overhead categories were staff wages, rent, and consumables — not technology depreciation.
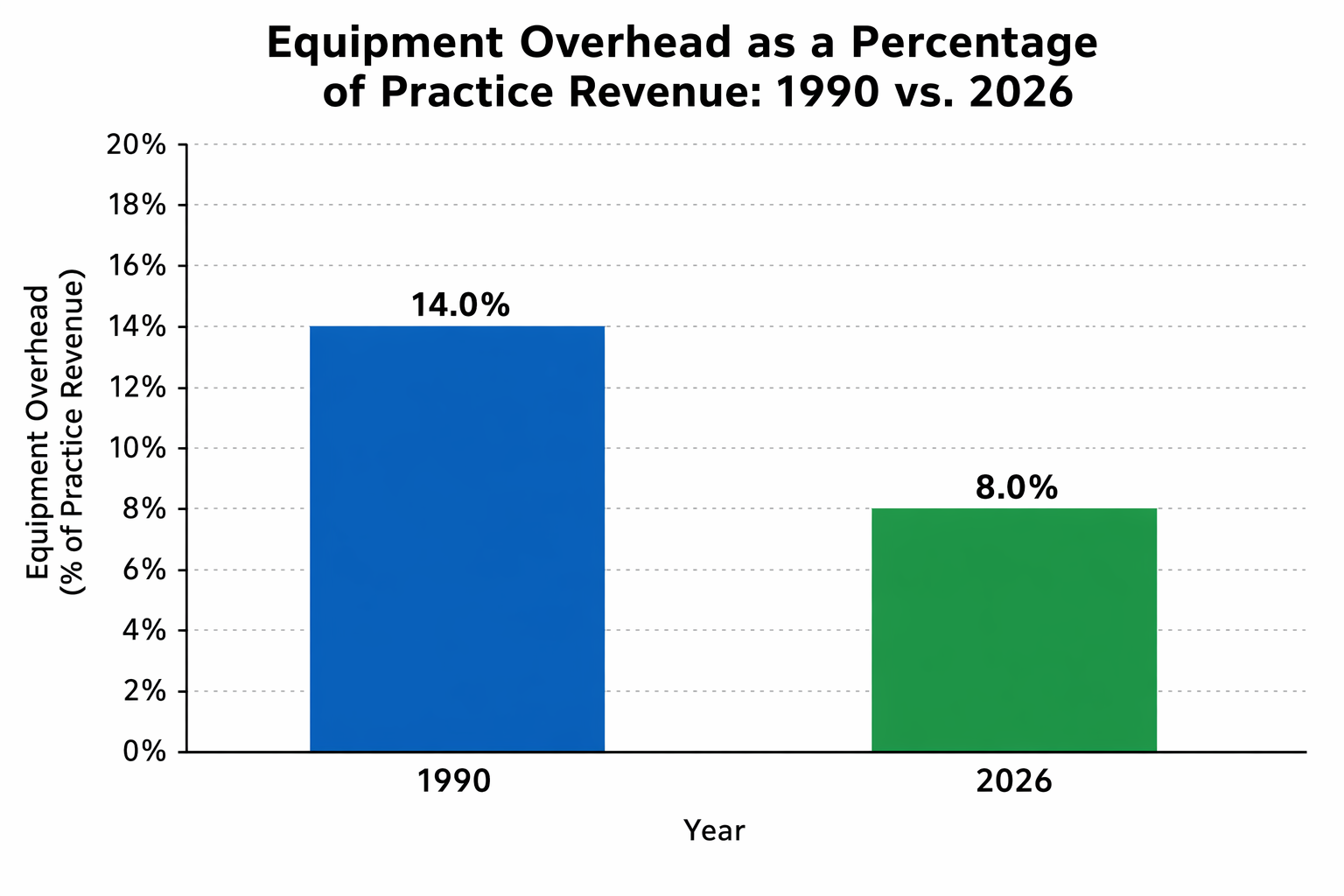
Industry surveys from that era consistently placed equipment-related overhead at roughly 5–7% of gross revenue for a typical general practice. The rest was labour (roughly 25–30%), facility costs, and materials. The cost per clinical minute was driven almost entirely by how many patients could be scheduled and how efficiently the dentist worked with simple tools.
02The Technology StackWhat Practices Now Carry on the Balance Sheet
The transformation did not happen overnight. It came in waves: digital radiography in the late 1990s, implant systems through the 2000s, CBCT and intraoral scanners through the 2010s, and AI-assisted diagnostics and digital workflows now. A 2020 survey of US dentists — published in JDR Clinical and Translational Research — found that digital imaging, dental implants, and adhesive materials were rated as the three most practice-altering innovations of the preceding 30 years. Each of those innovations also carries a significant capital and running cost.
A rough inventory of a fully equipped general practice in 2026 might look like this:
- Intraoral scanner (€15,000–€30,000 purchase + annual software subscription)
- CBCT unit (€60,000–€120,000 purchase + maintenance contract)
- CAD/CAM milling unit (€30,000–€80,000 + bur replacement + service)
- Digital radiography system (€10,000–€25,000 per operatory)
- Electric handpiece system (€3,000–€8,000 per unit)
- Laser (€8,000–€40,000 depending on type)
- Practice management software (monthly SaaS fees + hardware)
- Intraoral cameras (€1,500–€5,000 per unit)
Spread across a 10-year depreciation horizon and factoring in maintenance, a fully digital practice can carry €15,000–€30,000 per year in technology-related fixed costs that simply did not exist in 1990. For a practice running 200 clinical days per year and 7 productive hours per day, that translates to an additional €10–€21 per clinical hour in fixed overhead — before a single patient sits in the chair.
03The Cost Per MinuteRunning the Numbers
The concept of "cost per minute" is a useful forcing function for practice economics. It asks: what does it cost the practice for every minute the dental chair is occupied — or, more painfully, unoccupied?
If a practice's total annual overhead (staff, rent, materials, equipment, software, insurance) runs to €400,000 and the practice generates 1,400 productive clinical hours per year, the cost per minute is approximately €4.76. A 30-minute hygiene appointment needs to generate at least €143 just to break even on direct costs — before the dentist's own income is factored in.
Technology raises this floor. Add €20,000 per year in equipment depreciation and service contracts, and the cost per minute rises by roughly €0.24 — a number that sounds small but compounds across every appointment, every day, every year. For a practice doing 4,000 appointments annually, that is an additional €48,000 in revenue that must be generated simply to stand still.
The chair that sits empty is the most expensive piece of equipment in the practice.
Practice management principle — widely cited in dental business literature
04The Other Side of the LedgerWhen Technology Pays for Itself
The cost argument only holds if technology delivers no return — and that is rarely true. The same innovations that raise overhead also change what is clinically possible and how efficiently it can be delivered.
An intraoral scanner eliminates impression material costs, reduces remakes, and shortens appointment time for crown preparation workflows. A CBCT unit enables implant planning that reduces surgical complications and supports same-day treatment decisions that would otherwise require referral. CAD/CAM same-day restorations eliminate the temporary crown appointment and the second cementation visit — compressing two appointments into one and freeing chair time for additional patients.
The honest accounting is not "technology costs more" but rather "technology costs more and changes the revenue per hour if the practice is structured to capture that value." A practice that owns a CBCT but refers all implant cases to a specialist is paying the capital cost without capturing the clinical return. A practice that integrates CBCT into a full implant workflow — planning, surgery, restoration — is amortising the same device across a much higher revenue base.
05The Strategic QuestionInvestment vs. Overhead
The practices that manage technology costs most effectively treat equipment acquisition as a strategic decision, not a catalogue purchase. The key questions before any major acquisition are straightforward: How many procedures per month does this device enable or accelerate? What is the realistic revenue per procedure? At what monthly utilisation rate does the device break even against its annualised cost?
A CBCT unit at €80,000 purchase price, €3,000 per year in maintenance, and a 10-year depreciation horizon costs roughly €11,000 per year. If the practice charges €150 per CBCT scan and performs 10 scans per month, the device generates €18,000 per year — covering its cost and contributing margin. At 5 scans per month, it runs at a loss. The device is identical in both scenarios. The economics are determined entirely by utilisation.
06Looking ForwardThe Practices That Will Win
The gap between a 1990 practice and a 2026 practice is not just technological — it is financial in structure. Modern practices carry higher fixed costs, require more capital, and demand more sophisticated management to remain profitable. That is not a reason to avoid technology. It is a reason to be deliberate about which technology to adopt, when, and at what utilisation target.
The practices that will navigate this well are those that track their cost per minute, model the break-even utilisation for each device before purchasing, and build clinical workflows that maximise the revenue-generating potential of every piece of equipment on the floor. The ones that will struggle are those that buy technology because competitors have it — without a plan to use it at the volume that justifies the cost.
Progress has a price. In dentistry, that price is now built into every minute of every appointment. The question is whether the practice is charging accordingly.

👨⚕️ doc. MUDr. Radek Mounajjed DDS., PhD. 🦷 D.C.M. Clinic 🎓 Associate Professor, Palacký University Olomouc, Czech Republic 📚 CICERO Cofounder ⚖️ Certified Court Expert in Dentistry
View educator profile