
It was 1993 when Mahmoud Torabinejad at Loma Linda University first described a material that endodontists had simply never had before. He called it mineral trioxide aggregate — MTA. At the time it sounded like a laboratory curiosity. Today it is one of the most frequently cited materials in the entire dental literature.
01The BasicsWhat MTA Actually Is
MTA is a calcium-silicate cement — at its core a modified Portland cement enriched with bismuth oxide, which gives it radiographic visibility. When it comes into contact with tissue fluid, it hydrates and forms hydroxyapatite. It is precisely this ability — to mineralize the interface between the material and living tissue — that is the key to its reputation.
The point is not that MTA is "strong" in a mechanical sense. The point is that it behaves biologically. It stimulates osteoblasts, cementoblasts, and pulp cells to form hard tissue. The body does not perceive it as a foreign body — it perceives it as a signal to heal.
02Why It WorksThree Properties That Make the Difference
Research has identified three properties that set MTA apart from predecessors such as calcium hydroxide or amalgam:
- Sealing ability. MTA exhibits minimal microleakage. Bacteria cannot get past correctly applied MTA — not even in the conditions of a moist environment, where other materials fail.
- Biocompatibility. Studies repeatedly confirm that MTA does not provoke an inflammatory response in the periapical tissues. On the contrary — it supports the regeneration of the original tissue, including cementum and periosteum.
- Alkaline pH. Freshly mixed MTA reaches a pH of around 12.5. This in itself inhibits bacterial growth and contributes to disinfection of the treated area.
03Where MTA Is UsedClinical Indications in Practice
MTA was originally designed for a single use: repair of root canal perforations. Today its list of indications is considerably longer.
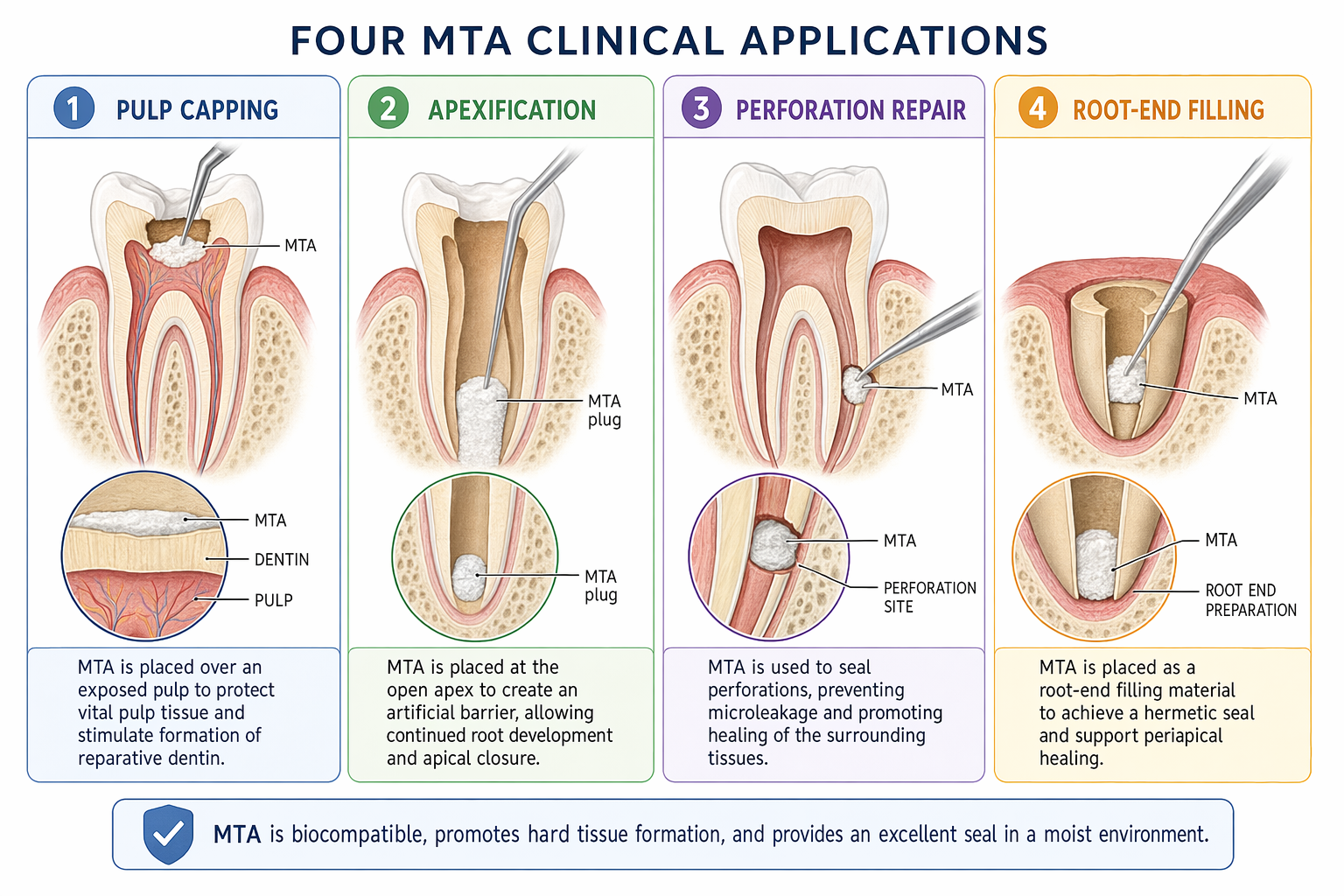
Direct pulp capping is now one of the most important applications. Where calcium hydroxide previously formed irregular dentin bridges with tunnels and defects, MTA induces the formation of compact, biologically high-quality dentin. Clinical studies show a markedly higher success rate in preserving tooth vitality.
Apexification and apexogenesis — in teeth with an immature apex and necrotic pulp, MTA makes it possible to create an apical barrier without months of waiting for calcium hydroxide. One visit instead of six.
Perforation repair — whether iatrogenic or resorptive, MTA is the material of first choice. Sealing ability and biocompatibility both play a role here.
Root-end filling in apical surgery — an MTA retrograde filling has become the standard of modern endodontic surgery. The results are consistently better than with amalgam or Super-EBA.
04The DownsidesWhat MTA Cannot Do
It would be dishonest to stay silent about the limitations. MTA has two well-documented drawbacks.
Long setting time — the original formulation set in 2–4 hours. This complicates clinical workflow and requires a temporary filling. Newer materials (Biodentine, various MTA variants) have shortened this time, but compromises in other properties remain.
Risk of discoloration — MTA can cause a greyish discoloration of the tooth, especially in the anterior region. The mechanism is linked to the oxidation of bismuth ions on contact with blood and light. White MTA formulations mitigate this problem but do not eliminate it entirely.
MTA is the material of choice for some clinical applications — despite its known drawbacks such as long setting time, high cost, and potential for discoloration.
Parirokh & Torabinejad · Journal of Endodontics, 2010
05Legacy and FutureWhy a Whole Generation of Bioceramics Rests on MTA
MTA opened the door to a whole family of calcium-silicate bioceramics — Biodentine, iRoot BP Plus, Bioaggregate. Each of these materials seeks to preserve the biological advantages of MTA while overcoming its practical limits.
But none of them would exist without the original breakthrough: the proof that a dental material can actively cooperate with the body instead of merely isolating it from it. That is the real magic of MTA — not chemical, but biological.

🌍 Cicero System🎓 Dental Education | 🛒 Procurement | 🏥 Clinic Management