
A dental office looks clean. Disinfection, sterilisation, single-use devices — all under control. But the air we breathe in it all day long escapes that control. Every time the turbine spins, every primer applied, every ceramic etched releases substances into the space that aren't visible — but they are there. And they stay.
01Invisible threatsWhat floats in the air of the operatory
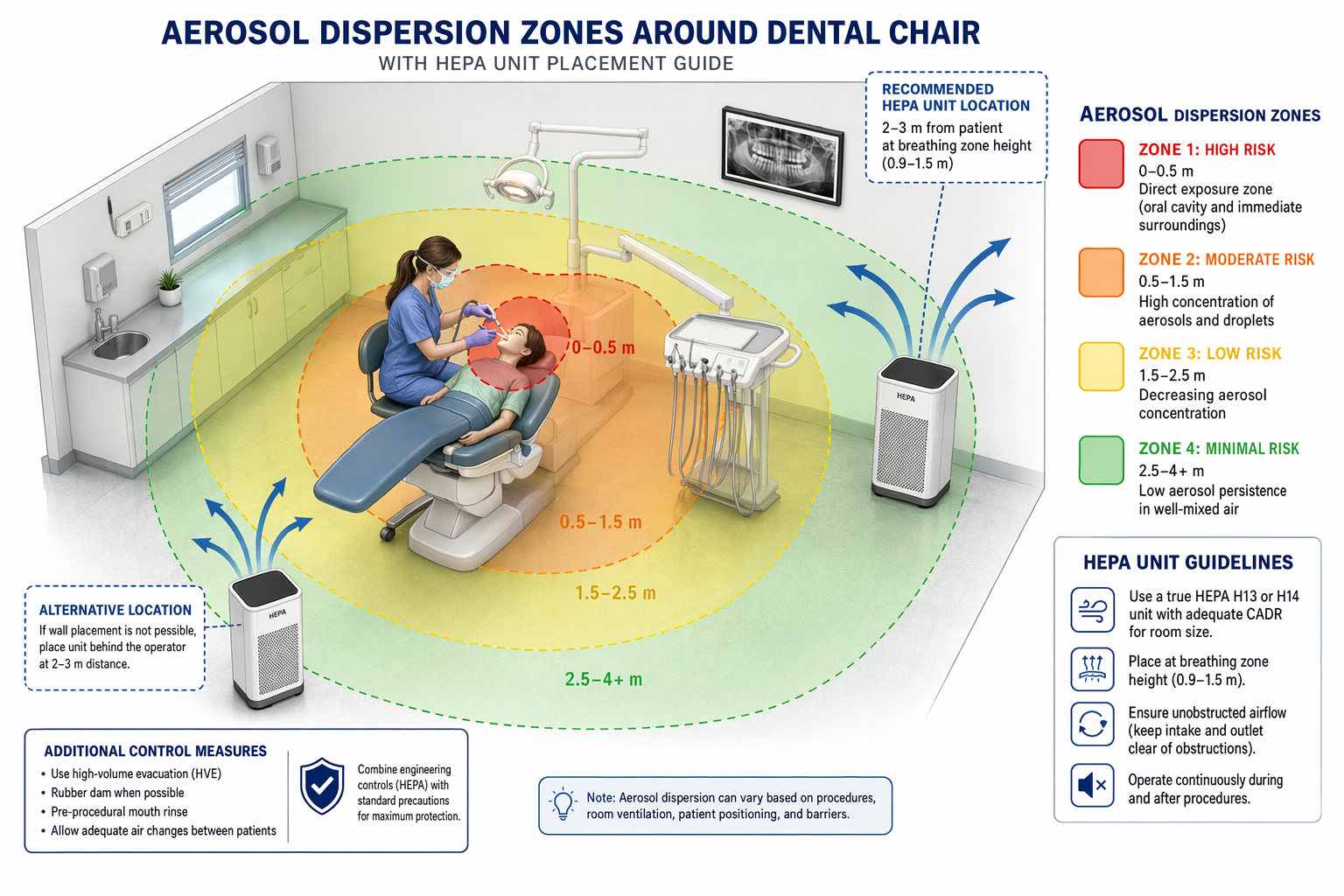
Working with a high-speed turbine or an ultrasonic scaler creates an aerosol — a mix of micro-droplets of water, saliva, blood and ground material. Particles smaller than 5 µm stay in the air for tens of minutes up to hours. They carry bacteria, viruses and fungi — whatever was in the patient's mouth.
A 2023 systematic review covering 42 controlled studies confirmed that bioaerosols from dental procedures represent a demonstrable infection-transmission risk in the operatory environment. Contamination spreads more than one metre from the procedure site and settles on surfaces and in the airways of everyone present.
Air-conditioning doesn't improve the situation — quite the opposite. In summer it recirculates the air inside the room without any real exchange. The HVAC filter catches dust but not microbial aerosol and not chemical vapour. The air gets cooled, but not cleaned.
02The chemistry we usePrimers, acids and monomers
Biological aerosols are only part of the story. Every day we work with substances whose chemical vapours are present in a closed operatory without us registering them.
Phosphoric acid (H₃PO₄) releases small amounts of vapour when etching enamel and dentin. When working with ceramics we use hydrofluoric acid (HF) — one of the most aggressive acids in the dental arsenal. Even at low concentrations it irritates the mucous membranes of the airways and repeated exposure damages lung tissue.
Monomers and primers are a chapter of their own. HEMA (2-hydroxyethyl methacrylate), bis-GMA, TEGDMA and MMA are found in bonding systems, composites, resin cements and provisional materials. Research from the Finnish Institute of Occupational Health has shown HEMA to be the most common allergen among dentists and assistants — contact dermatitis, but also reactive airway disease, are demonstrably linked to repeated exposure. A 2020 study published in the Journal of Esthetic and Restorative Dentistry called methacrylate sensitivity an "epidemically growing" problem in dental environments and pointed out that NIOSH (the US National Institute for Occupational Safety and Health) considers personal protective equipment insufficient — the primary solution must be environmental control.
Ceramic primers contain silanising agents and organic solvents. During application, part of them evaporates directly into the operatory air. The cumulative effect of daily exposure to low concentrations of these substances is well documented in the occupational-medicine literature.
Dental personnel need to be more aware of methacrylate sources and use workplace control measures to limit methacrylate exposures to both dental personnel and patients.
Bishop & Roberts · Journal of Esthetic and Restorative Dentistry, 2020
03Why HEPAFiltration that actually works
A HEPA filter (High-Efficiency Particulate Air) captures 99.97% of particles 0.3 µm and larger. That includes bacteria, viral aerosols and fine dust. Professional units combine HEPA filtration with activated carbon — which captures chemical vapours that HEPA on its own lets through.
A 2025 study published in the Journal of Hospital Infection tested portable HEPA+UV-C units directly in a dental environment. After 6 hours of continuous operation near the aerosol source, both tested units significantly reduced bioaerosol counts and improved the indoor-to-outdoor contamination ratio. The higher-efficiency model showed better capture of particles ≤ 5 µm — the most dangerous ones.
Placement is critical: the unit must stand as close to the aerosol source as possible, not by the door or in a corner. A single high-output unit is enough for a single-chair office; shared spaces or multi-chair practices need several.
04We only get one set of lungsWhy a mask alone isn't enough
An FFP2 mask protects against bioaerosols but does not catch the chemical vapours from monomers or silanes. Protective glasses don't prevent inhalation. Ventilation without filtration moves the air but doesn't clean it. A professional HEPA unit with activated carbon is the only device that addresses both axes at once — biological and chemical.
Long-term exposure to low concentrations of methacrylates, acids and bioaerosols doesn't build up into an acute event. It builds up into chronic sensitisation, allergies, reactive airway disease and repeated respiratory infections. A team that works in clean air works better, gets sick less often and lasts longer.
Investing in professional air filtration isn't a luxury for big clinics. It's a basic part of workplace safety — as obvious as the autoclave or protective gloves.

🌍 Cicero System🎓 Dental Education | 🛒 Procurement | 🏥 Clinic Management